30 year old male with DKA K/C/O Diabetes since 4 years Pulmonary TB 4 years ago
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs .This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
Patient was apparently asymptomatic till yesterday morning then he developed vomitings which are non bilious, non projectile, non blood tinged filled with food particles(10 episodes since yesterday which subsided from today morning). C/o loose stools 2 episodes yesterday morning which are watery, non blood tinged,non mucopurulent,not associated with fever, pain abdomen. C/o shortness of breath (grade 3) from yesterday evening which is not associated with chest pain, palpitations, orthopnea, pnd.
Patient was admitted in Gandhi hospital yesterday evening and was given IV fluids
And Inj.HAI 40iu.
Patient then came to our hospital due to shortness of breath
Past History:
He is a K/C/O DM since 4 years(was on insulin mixtard 10u-X-10u and was shifted to Tab.Metformin 500). He also has H/O Pulmonary TB 4 years ago (used ATT for 6 months)Tab. Glipizide 5 mg PO/BD from 1 week). H/O Pulmonary effusion(ICD was present for 10-15 days
Not a K/C/O HTN CAD CVA ASTHMA EPILEPSY THYROID DISORDERS.
Personal history:
Diet-mixed
Appetite-normal
Sleep-adequate
Bowel and bladder movements-regular
Addictions:90 ml whiskey thrice daily
Routine history:
Patient used to do centring work 4 years back then one day he had fever and increased urinary frequency and was lethargic so went to a local rmp and diagnosed to have diabetes, so he stopped doing centring work as he thought he might have injuries and may not heal. He didn't go to any work for 5 to 6 months because of fatigue and cough and diagnosed with TB ( he used 6 months mediation and was complient). Now he is working as mechanic.
Current daily routine:
He wakes up at 6 am and takes 10 U of HAI and has breakfast and goes to work and has lunch at 2pm and then goes around for a walking if he feels bloated and takes 10 U of HAI before having dinner at 8 pm and sleeps at 10pm.



General examination:
Patient is conscious, coherent and cooperative He is moderately built and moderately nourished
No signs of icterus, cyanosis, clubbing, lymphadenopathy, edema
Vitals:
Patient is conscious, coherent, cooperative.
Temp: 98.7F
PR- 106 bpm
RR-23cpm
BP-130/70 mm of Hg
Spo2 - 98%
GRBS:130mg/dl
Systemic examination:
PER ABDOMEN
Inspection:
No Abdominal distension
No scars, sinuses, mass visible
Palpation:
Inspectory findings are confirmed
No local rise of temperature
No Tenderness present
Auscultation:
Normal bowel sounds heard
RESPIRATORY SYSTEM EXAMINATION
Inspection:
Bilaterally Symmetrical chest movements present
No scars and sinuses
Trachea central
Palpation:
Inspectory findings are confirmed
Percussion:
Resonant note present in all lung areas
Auscultation:
Normal vesicular breath sounds heard.
CARDIOVASCULAR SYSTEM EXAMINATION
Inspection :
Bilaterally symmetrical chest present
No scars, sinuses
Palpation:
Inspectory findings are confirmed
Apex beat normal
On Auscultation :
S1 S2 heard, no murmurs or additional heart sounds
CENTRAL NERVOUS SYSTEM EXAMINATION
Higher mental functions intact
Cranial nerves intact
No focal neurological defecits
Provisional diagnosis
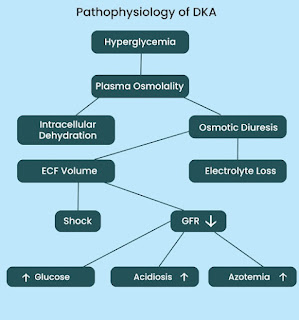
Diabetic ketoacidosis with K/C/O Diabetes since 4 years and Pulmonary TB 4 years ago
Investigations:
GRBS
15/7/2023
7pm 216mg/dl
8pm 180mg/dl
9pm 195mg/dl
10pm 209mg/dl
16/7/2023
12am 192mg/dl
1am 196mg/dl
2am 168mg/dl
3am 157mg/dl
5am 153mg/dl
6am 132mg/dl
7am 130mg/dl
8am 112mg/dl
10am 116mg/dl
12pm 126mg/dl
2pm 128mg/dl
4pm 135mg/dl
6pm 142mg/dl
8pm 252mg/dl
10pm 295mg/dl
17/7/23
12am 185mg/dl
2am 194mg/dl
4am 220mg/dl
6am 179mg/dl
8am 170mg/dl



Treatment:
16/7/23
1.IV Fluids 0.4%NS IV @250 ml/hr
2.Inj.Hai 40u in 39 ml NS @ 2.5 ml/hr
3.Inj.5%Dextrose @100 ml/hr according to GRBS
4.Monitor grbs hourly
5.Monitor vitals second hourly
6.strict I/O charting
17/7/23
1.Inj.nph s/c BD premeal according to GRBS
2.Inj.Hai s/c TID premeal according to GRBS
3.Grbs 7.profile monitoring
4.Monitor vitals fourth hourly
5.strict I/O charting


Comments
Post a Comment