Short case
K.Shubankar
1701006169
This is an E logbook to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here, we discuss our individual patient's problems through series of inputs from an available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence-based inputs. This E-logbook also reflects my patient-centered online portfolio and your valuable inputs in the comments are welcome.
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
A 25 year old female patient who is a housewife and resident of Miryalaguda came to OPD with cheif complaints of
CHEIF COMPLAINTS:
High blood pressure ( came for checkup )
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 1 year back then she developed hypertension which was found out on her 1 St pregnancy. She had 2 abortions in the past i.e in 1 year back in 2021 and 5 months back in 2022 .Her obstetric formula is P2A2L0.
In 1st pregnancy i.e 1 year back in 2021 when the patient conceived she visited obstetrician and found out to have hypertension which was 150/100 mmhg.She had history of pedal edema. She was started on anti hypertensive drugs i.e tablet labetalol 100 mg PO BD. At around 8 months, patient had Intrauterine death of fetus and baby was delivered by normal vaginal delivery.
Then she stopped taking anti hypertensive drugs.After a gap of 3 months she conceived again in 2022.
In 2nd pregnancy i.e 5 months back in 2022 she conceived and found out to have hypertension which was160/100mmhg. She was started on anti hypertensive drugs i.e tablet labetalol 100mg PO BD. At around 8 months preterm delivery which was done by normal vaginal delivery, the baby died within 1 day.
Now the patient has no history of palpitations, shortness of breath, pedal edema, decreased urine output, headache, blurring of vision.
PAST HISTORY:
History of hypertension since one year
No history of Diabetes mellitus, Tuberculosis, Asthma, CAD
No history of blood transfusion
No history of previous surgeries
TREATMENT HISTORY:
History of usage of anti hypertensive drugs i.e labetalol.
PERSONAL HISTORY:
Diet : Consume both Veg and Non-Vegetarian foods
Appetite: normal
Bowel and bladder : regular
Sleep : adequate
No addictions
No allergies
FAMILY HISTORY:
No significant family history.
GENERAL EXAMINATION:
After taking informed consent the patient was examined in a well lit room.
On Examination: Patient is Conscious, Coherent and Cooperative well oriented to time, place and person
Clubbing - absent
Pallor - absent
Icterus - absent
Cyanosis - absent
Edema of feet - absent
Lymphadenopathy - absent
VITALS:-
On admission i.e on 8-6-22 :
Temperature: afebrile
BP: 170/100 mm hg
PR: 90 bpm
RR: 22 cpm
SPO2: 98%
GRBS: 164 mg%
On 11-6-22:
Temperature: afebrile
BP: 160/100mmhg
PR: 98 bpm
RR: 16 cpm
On 12-6-22 :
Temperature: afebrile
BP: 120/80mmhg
PR: 74 bpm
RR: 16 cpm
SYSTEMIC EXAMINATION :
CARDIOVASCULAR SYSTEM :
S1 and S2 heard, no murmurs heard
RESPIRATORY SYSTEM :
BAE present, NVBS heard, position of trachea - central
PER ABDOMEN :
soft, non tender.
No organomegaly.
CNS:
Higher mental function intact,NAD.
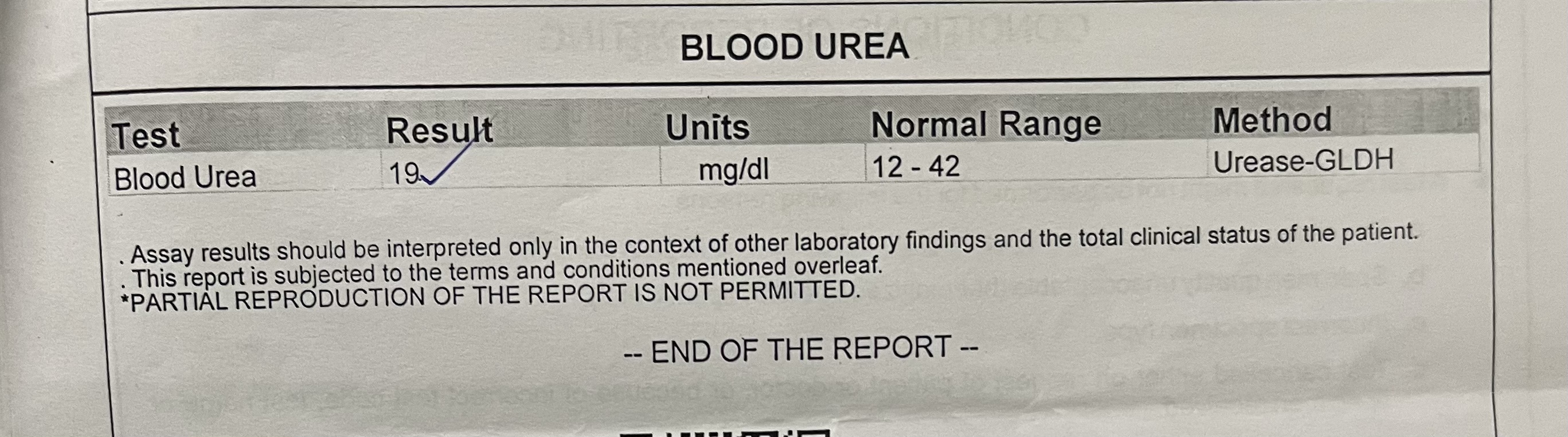
INVESTIGATIONS:
Blood urea : 19
Serum creatinine: 0.8
CBP
Hb: 14.1
TLC: 9,900
Neutrophils: 65
Leucocytes: 30
PCV : 40.4
MCV: 85.4
MCHC: 34.9
Platelet count: 3.64
RBC: Normocytic normochromic
Ultrasound Abdomen
On 8-6-22:
Na - 142
K - 3.8
Chloride- 103
Complete Urine Examination:
Albumin- trace
LFT:
SGOT: 20
SGPT: 30
ALP: 218
Total Protein: 7.6
Albumin: 4.18
A/G ratio: 1.22
Thyroid Profile:
T3- 1.32
T4- 10.75
TSH- 2.32
Lipid Profile:
Total cholesterol-204
Triglycerides-201
HDL- 55
LDL-120
VLDL-40.2
Chest X-ray:
PROVISIONAL DIAGNOSIS:
YOUNG ONSET HYPERTENSION
TREATMENT:
1) Tablet. AMLONG 5 mg PO OD
2) Tablet. Zincovit PO OD.











Comments
Post a Comment